
Case Report | DOI: https://doi.org/10.31579/2692-9392/036
1 Department of Neonatology, The Hospital of the First Affiliated Hospital, Sun Yat-sen University, Guangzhou 510080, Guangdong, China.
*Corresponding Author: Xiao-ping Luo, Department of Neonatology, The Hospital of the First Affiliated Hospital, Sun Yat-sen University, Guangzhou 510080, Guangdong, China.
Citation: Li Wang, Xiao-ping Luo, Yan-wei Liu (2021) Hepatic Lesions of Total Parenteral Nutrition (Tpn) Secondary to Umbilical Venous Catheter (Uvc) Malposition in A Very Low-Birth Weight Infant in China. J. Archives of Medical Case Reports and Case Study. 4(2); DOI: 10.31579/2692-9392/036
Copyright: © 2021 Xiao-ping Luo, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 February 2021 | Accepted: 19 April 2021 | Published: 26 March 2021
Keywords: umbilical vein catheterization; hepatic lesions; nutrition; Tpn; UVC; GBS; NEC
Umbilical vein catheterization (UVC) is a common operation for vascular access in preterm infants. However, there are complications associated with their use. We here a case of extravasation of the fluids due to misplacement of the catheter causing hepatic collection of TPN in a very low-birth weight preterm (VLBW) infant.
Umbilical vein catheterisation (UVC) is a commonprocedure performed in neonatal intensive care unit (NICU) [1]. UVCs allow quick access for intravenous fluid and drug administration, blood products and parenteral nutrition to acutely ill neonates; besides these benefits, there are complications associated withtheir use[2-4]. One of uncommon complication is extravasationof the fluids due to misplacement of the catheter. Inapposite position ofUVCs can sometimes cause such leakage into theliver tissue with significant damage to the liver parenchyma or lead to necrosis of the area [3, 5].We present a case of preterm baby who developed partialnecrosis of liverfollowing a malposition UVC with successful recoveryfollowing discontinuation of the catheter and abdominal paracentesis of the fluid.
This female neonateweighing 1.42kg, was born at 36 1/7 weeks of gestation, after 8 hours of ruptured membranes, by vaginal delivery.There was nohistory of maternal hypertension or diabetes. The mother has regular prenatal examinations during pregnancy. GBS screening negative. After birth, Apgar score is good. But thebaby had poor respiratory efforts at one hour after birth requiringnasal continuouspositive airway pressure (nCPAP) and non-invasiveventilation. For vascular access, a 3.5 Fr double lumen UVC were inserted uneventfully. The tip of the catheter was placed to the right of the vertebral column, at the level of T10 vertebra, below the level of the diaphragm (Figure 1A).

The UVC were used for all infusions, including TPN.
On day 3 of life, the patient showed signs of sepsis with temperature instability, dyspnea, circulatory system instability and increased serum inflammatory parameters (CRP 22.8 mg/l, reference range <8 mg/L). Vancomycin (20 mg/kg q12 h) and piperacillin-sulbactam (75 mg/kg q8 h) were started. On day 5, she received a single dose of intravenous immunoglobulin (1 g/kg). On day 6 of life, abdominal distension developed. The radiography revealed a gasless abdomen (Fig. 1B) and abdomen ultrasonography revealed significant amount of free fluid but no pathology at the liver.

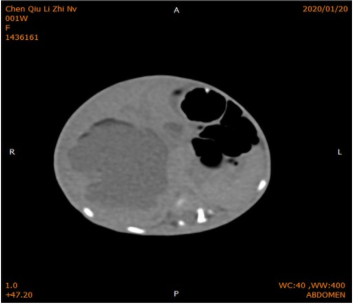
There was no evidence of any perforation or necrotising enterocolitis (NEC). On day 9 of life, the signs of sepsis did not improve and the laboratory tests showed an elevated CRP (69.9 mg/l) thrombocytopenia, abnormal liver enzymes (ALT 199U/L, reference range <40 U/L) and coagulation defects. A CT scan demonstrated a 5.3-cm complex air-containing fluid collection in the liver (Figure 2).
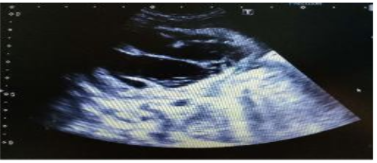
Ultrasound (US) examination of the abdomen showed fluid collection in the liver (Figure. 3a).
The UVC was removed and a peripherally inserted central catheter (PICC) was placed. Antibiotics were changed to meropenem (20mg/kg, q12h) in view of the worsening clinical condition and to provide a wider antimicrobial coverage. She received normal saline boluses, fresh frozen plasma and other blood products during this period. In view of the critically ill state of the infant, the surgeons performed an US-guided hepatic collection aspiration by inserting a Penrose drain to relieve the abdominal pressure. Approximately 60 ml of milky-looking fluid was drained. Fluid analysis indicated triglycerides consistent with TPN. Following paracentesis, the baby’s condition improved significantly.
The US examination of the abdomen 3 days post-hepatic collection aspiration revealed collection of fluid in the liver. The liver showed a solid-cystic echogenic lesion measuring 3.6×2.8cm with internal visible separation (Figure 3b).
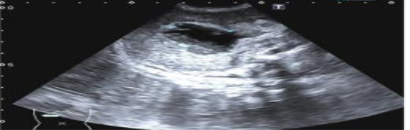
The surgeons performed an US-guided hepatic collection aspiration without fluid withdrawal and recommended conservative treatment. At 11 days later, the patient developed fever again. Subsequently, repeat US examination showed the lesion do not have been absorbed measuring 3.0×2.3cm with no vascularity (Figure. 3c).

The surgeons performed again an US-guided hepatic collection aspiration. Repeat follow-up US examination at 2 weeks later demonstrated the lesion to have decreased to 2.5×0.9cm with a hyperechoic lesion (likely from calcium in the lesion). On day 27 of life, the baby cured and discharged. A CT scan, performed at day 44 of life (17 days after discharge) for follow-up of these lesions revealed a 1.3-cm punctate low density shadow in the left lobe of the liver. At 7 months of age, a follow-up US revealed dystrophic calcifications in areas previously described as abnormal fluid accumulation in the liver (Figure 3d).

This case showed that the UVC was improperly placed and prolonged parenteral nutrition infusion, which the entry of hypertonic fluid into the liver tissue may lead to parenchymal injury or parenchymal necros. This was consistent with previous reports [4-5]. UVC is a commonly used procedure in the NICU. However, great care must be taken to ensure proper placement to prevent possible short-term and long-term complications. The tip of the umbilical catheter must be placed over the diaphragm, at the junction of inferior vena cava and right atrium corresponding to T9 [5-6]. Since UVC is placed by estimating (shoulder-umbilical length) rather than confirming the placement process in real time, UVC may inadvertently enter the portal vein system during placement. In addition, it is possible to transfer the tip of the venous catheter into the portal vein, even at the appropriate initial location. Hence, it is important to emphasize that UVC placement in the inferior vena cava is necessary, although the ideal location is the inferior vena cava/right atrium confluence.
The confirmation of the location of the UVC tip is usually done with radiography. But a recent study has shown that x-rays often do not accurately locate UVC in premature infants and real-time US or echocardiography is a more accurate technique to determine the appropriate location of UVC tip [7]. Although UVC should be removed as soon as possible, it can be retained for up to 14 days if the catheter placement is appropriate [8].
Our cases demonstrated the effectiveness of this method, US-guided drainage and the necessity of multidisciplinary combined treatment for acute and severe cases. The prognosis of this case is good. Although the use of UVC is part of the daily management of the NICU, it is important to be aware of their potential complications and to monitor their location with X-ray or US study. Catheter-related complications must be considered whenever there is acute abdominal distension with UVC in place.
The malposition of the UVC is the most likely to occur hepatic collections/necrosis. The position of UVC should be carefully monitored by regular x-rays or bedside ultrasound. Abdominal distension with UVC should cause suspicion of total parenteral nutrition hepatic collection. Liver ultrasound is the best way to diagnose newborns with parenteral nutrition infiltration of the liver. Generally, if managed appropriately, the prognosis of this condition is good.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
